

Formulario de solicitud de autorización previa de medicamentos recetados o excepción de terapia escalonada
Utilice este formulario para enviar solicitudes de autorización previa de medicamentos recetados para miembros de Alliance Care IHSS. Envíe un fax a MedImpact al (858) 790-7100. Si tiene alguna pregunta, comuníquese con MedImpact al (800) 788-2949.
Para solicitudes de autorización previa de medicamentos recetados para miembros de Medi-Cal, consulte www.Medi-CalRx.dhcs.ca.gov.
Medicamentos administrados por un médico
Utilice este formulario para enviar solicitudes de autorización previa para medicamentos administrados por médicos a la Alianza. Envíelo por fax al Departamento de Farmacia de la Alianza al 831-430-5851. Para obtener más información, consulte Medicamentos administrados por médicos (para Medi-Cal e IHSS) - Central California Alliance for Health.
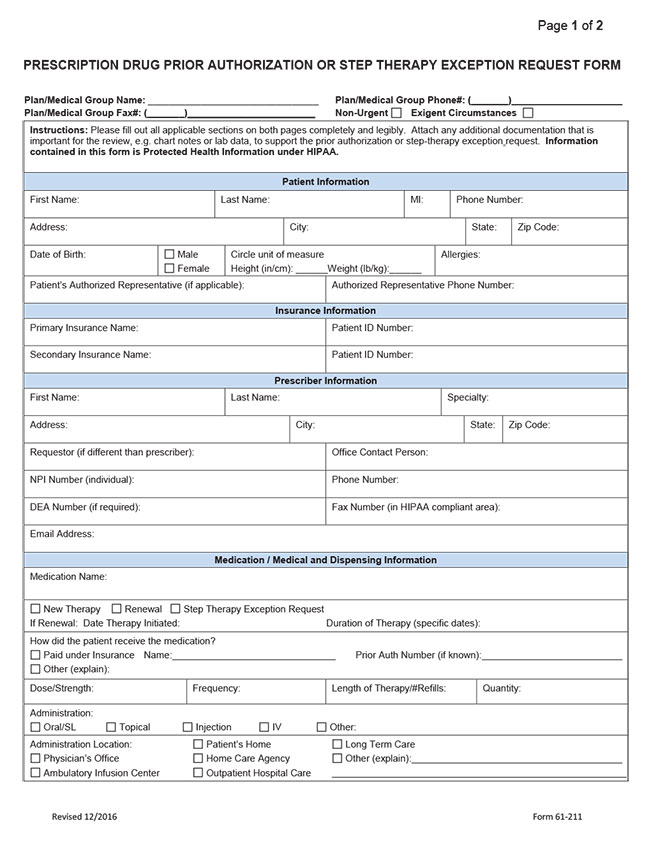
Haga clic en la imagen a continuación para abrir el archivo de PDF:
Contactar con el Departamento de Farmacia
Teléfono: 831-430-5507
Fax: 831-430-5851
De lunes a viernes: 8 a. m. a 5 p. m.
Recursos para proveedores
Últimas noticias sobre proveedores





Recursos Para Miembros

© 2026 Alianza para la Salud del Centro de California | Comentarios del sitio web