

Prescription Drug Prior Authorization or Step Therapy Exception Request Form
Use this form to submit prescription drug prior authorization requests for Alliance Care IHSS members. Fax to MedImpact at (858) 790-7100. For any questions, contact MedImpact at (800) 788-2949.
For prescription drug prior authorization requests for Medi-Cal members, refer to www.Medi-CalRx.dhcs.ca.gov.
Physician-Administered Drugs
Use this form to submit prior authorization requests for Physician-Administered Drugs to the Alliance. Fax to the Alliance Pharmacy Department at 831-430-5851. For more information, refer to Physician-Administered Drugs (for Medi-Cal and IHSS) - Central California Alliance for Health.
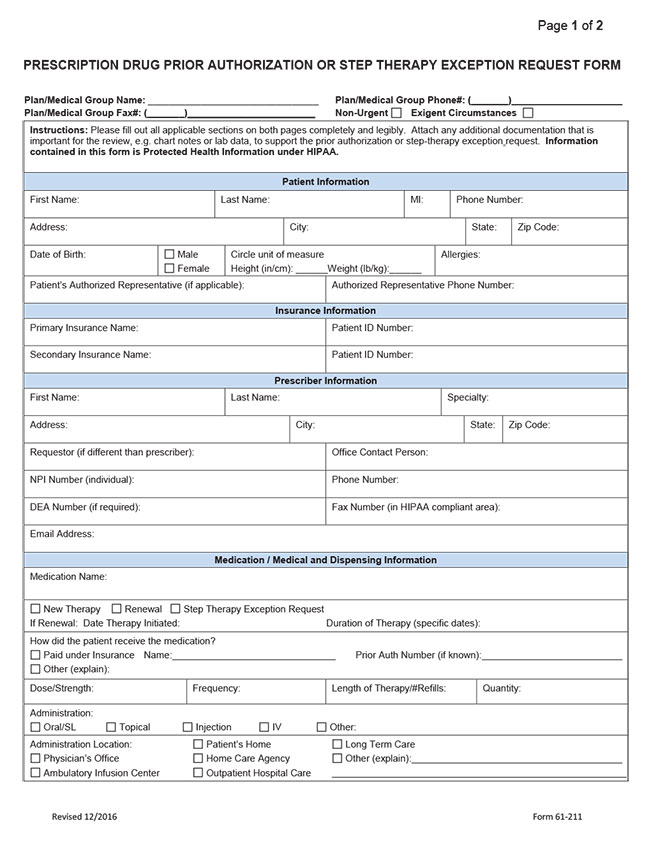
Click image below to open PDF file:
Contact Pharmacy Department
Phone: 831-430-5507
Fax: 831-430-5851
Monday-Friday, 8 a.m. to 5 p.m.
Provider Resources
Latest Provider News





