

Tus txheej txheem Reimbursement Rate Request
Cov neeg muab kev cog lus tuaj yeem siv daim foos no los thov cov ntaub ntawv them rov qab los ntawm Alliance. Thov nyeem cov lus qhia tab kom tag nrho ua ntej sau thiab xa daim foos. Cov kws kho mob uas tsis tau cog lus nrog Alliance yuav tsis siv daim ntawv no, tab sis yuav tau txais Medi-Cal tus nqi ntawm Department of Healthcare Services DHCS lub website.
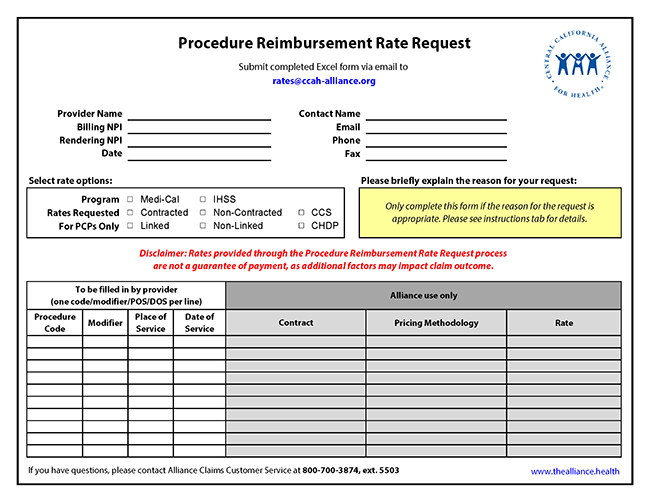
Nyem duab hauv qab no kom qhib Excel cov ntaub ntawv:
Hu rau Pharmacy Department
Xov tooj: 831-430-5507
Fax: 831-430-5851
Monday-Friday, 8 teev sawv ntxov txog 5 teev tsaus ntuj
Muab Kev Pabcuam
Xov Xwm Tshaj Tawm Tshiab





